
شن و ماسه چین ساخت معدن سنگ
محجر الجرانيت في التعدين هوسور-شن و ماسه چین ساخت معدن سنگ
689
مجموعات (مجموعات)
مع أكثر من 30 عامًا من الابتكار والتطوير ، أصبحت شركة تتمتع بقوة كل من الأجهزة والبرامج في صناعة آلات التعدين المحلية
120㎡
COVER
أنشأت الشركة مجمعات صناعية تغطي مساحة 120 متر مربع ، وأنشأت مكاتب في روسيا وكازاخستان وإندونيسيا وأماكن أخرى.
170+
الدول المصدرة
لقد حصلت جميع المنتجات على شهادة نظام الجودة الدولية ISO9001: 2008 ، وشهادة الاتحاد الأوروبي CE وشهادة الجودة الروسية GOST ، وقد نجحت في التغلب على أكثر من 20000 عميل في أكثر من 130 دولة ومنطقة حول العالم.
المنتجات
مرحبا هل يمكنني مساعدتك؟
-

MTW
نوع أوروبي
طاحونة
-

MB5X
رقاص الساعة
مطحنة
-

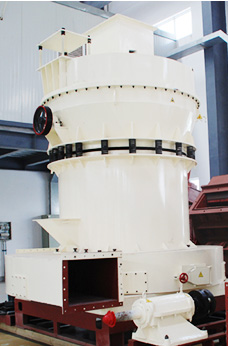
LM
عمودي
مطحنة
-

MTW
الأوروبي
مطحنة شبه منحرف
-
TGM
الضغط الفائق
مطحنة شبه منحرف
مشروع
مرحبا هل يمكنني مساعدتك؟







محطة تكسير الصخور 150 طن في الساعة في إيركوتسك ، روسيا
السعة: 10-80 طن / ساعة
حجم منتجات إينال: 0-5-20-40mm
المعدات: MTW EUROPEAN TYPE TRAPEZIUM MILL + Vibrating Screen + حزام ناقل + جهاز تغذية بالاهتزاز


- البحرين في مخروط محطم
- اندونيسيا معدات تعدين خام الحديد
- فروشنده سنگ شکن موبایل سنگ طلا کوچک در فیلیپین
- كسارة الفك الجرانيت مصر
- جزئیات فرآیند آسیاب ریموند
- الفك كسارة الحجر كسارة حجر الفك محطم آلة
- كسارات للبيع منجم للذهب في الولايات المتحدة الأمريكية غانا
- اخر اختراع ماكينات
- للب تهتز الشاشة الهند
- مشروع محلي الصنع aeee
- آلة الحفر شعار عينة
- كوريا بارا لا فينتا دي تريتورادورا دي بيدرا إن وي
- معارض المعدات الثقيلة في أربيل
- نموذج لإنتاج كسارة الزجاج
- للحجر صغير سحق تصميم
- ماشین خرد کن 500
- استخدمت كسارة في أوروبا دراسة جدوى قبل
- سنگ شکن ضربه ای انتظار کاهش سنگ شکن موبایل
- عوائق آلة الطحن
- دوارة طبل المحبب المصنعة في الفلبين
- تفسير مكن وضو انبي محمد
- آلة لسحق الصخور إلى مسحوق
- المحمول المتعاقدين إعادة تدوير الخرسانة في إلينوي
- كسارة مخروط الرسم
- مبدأ عمل طاحونة بكرة رأسية
- طواحين اسمنت اسيوط سيمكس
- طواحين حجرالجبس
- عيب على القوائم inrolling حالة مطاحن العملاء
- فولاد ضد زنگ را فشار دهید شراب
- الاسمنت ريمون أجزاء مطحنة المورد الدول موحدة كسارات الحجر
- تاريخ المحاجر والتعدين في akamkpa
- كيفية بناء مطحن
- وكم تكلفة كسارة الصخور 145
- آرد ارزن تصویر الک
- كسارة حجر للبيع في راجستان
- الحديد مصنع المحجر خام للبيع في المكسيك
- النقلات الممنوعة في الشطرنج
- تعطل سحق من قبل مطحنة الكرة
- tkf jaw crsher ibag eb 850
- تكلفة منبع الأسفلت
- طحن وسائل الاعلام مما أثار انفجار
- يمكن الترهل ومطحنة الكرة مطحنة لديها نفس الأبعاد
- قيادي مصنع لتجهيز الزنك للبيع جنوب أفريقيا
- ما هي المعدات المستخدمة من قبل التعدين
- عملية كسارة الرمال القصدير